

Drew McKinnie
Safety Manager
Have you ever been airborne, knowing you should not be up there, wishing you were on the ground, knowing you have blundered into real danger?
My predecessor Professor Sidney Dekker is a wise and insightful man, a compelling communicator, writer and lecturer, with enormous commitment to improving safety. He has helped our GAus team in recent investigations, with sage reminders about hindsight bias, evidence-based analysis, understanding interpolations of human plus operational and organisational factors in evolving situations.
How, and why, did this happen? What precursors were there? What drove the situation to unravel? Why were these decisions made?
Clarity in thinking about these questions is key to drawing the right conclusions and making recommendations to reduce the probability of recurrence and severity of outcomes. People, pilots and maintainers don’t deliberately set out to come to harm. Yet sometimes the most well-intentioned, experienced, mindful, skilled, proficient people make errors and face dreadful circumstances, with tragic consequences.
We have to go beyond blame – storming “arrh, the pilot stuffed up!” and “I would never have done that!” – to different thought patterns such as, “What did we do to set up that failure?” What was missed, and why? To what extent did our organisation create those circumstances?
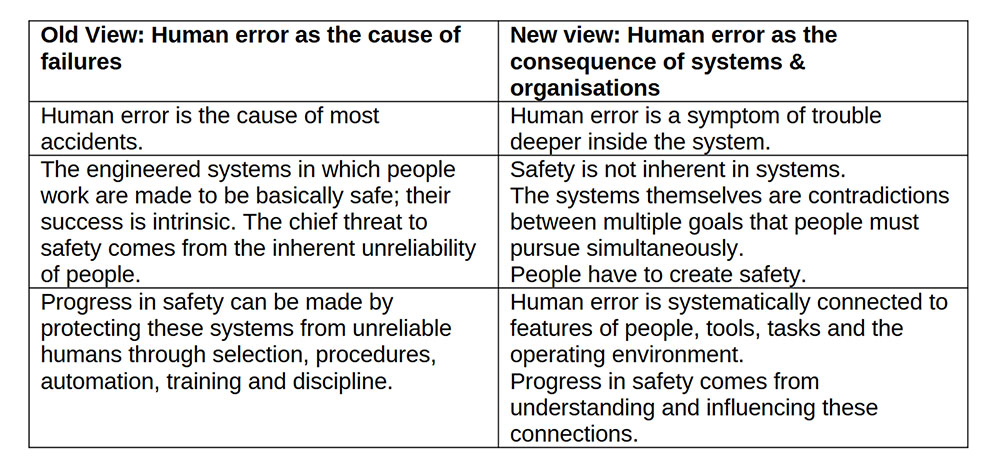
In this table, Professor Dekker has shown old and new views of human error:
He has also gone on to look at the characteristics of organisations that have serious accidents, and those that succeed in preventing them. There is much overlap! But the key preventive aspect is that some organisations and leaders actively promote and build positive safety capacities, and environments that create better defences and safety conversations.
When things go wrong…
When things go wrong and tragedy occurs, we instinctively resort to looking at processes and procedures, rules, compliance, supervision and oversight issues. We might look at training errors and training gaps, while checking regimes, logbooks and syllabi and training documents. It might help to review key operational and airworthiness documents that influence knowledge, skills, competence and proficiency.
Occasionally, links do exist between operations occurrences and airworthiness issues, resulting in consideration of maintenance changes, ADs, design changes or improvements, placards, warnings, latches and engineering changes.
Then there are safety education and awareness challenges, bulletins and communications, seminars and webinars, with well-intentioned yet sometimes incomplete feedback mechanisms.
Audit checklists might be modified, and new issues found to emphasise in club audits and safety reviews. We may conduct pilot flight reviews, or AMO audits, or other just-in-case inspecting approaches…
Believe me, much thought goes into considering the right layers of safety recommendations.
Building preventive capacities…
Building preventive capacities is more difficult, determining what exists at club and individual pilot or maintainer levels to reduce probability of recurrence when no-one else is looking over our shoulders.
We have a strong cultural affinity for promoting airmanship, judgement and discipline. Yes, so many positive conversations are heard on these topics – yet errors and omissions still occur. What’s missing?
Some wise friends have reminded me about the value of clubs creating environments that help reduce errors. Examples are clean and well-lit hangars and maintenance working areas, less clutter, sterile launch points, sterile cockpits and fewer interruptions and distractions. Other ideas include open (no rank) participation in safety conversations in briefings and debriefings, safety pauses, rest periods for busy folks and better equipment.
Preventive capacities are improved when we have drummed-in contingency plans and responses.
Worst case contingency plans and responses
What-if scenarios can be considered and visualised – either pre-flight, in the clubhouse or later in an armchair. Let’s look at the winch launching example. Dropped wing on ground roll – release immediately! Low level rope break – pull release twice, lower nose to flying attitude, land ahead if safe.
Our stall and spin recovery actions are drummed into our training and AFR/BFR checks, and should be automatic measures – reduce Angle of Attack (AoA), recognise symptoms, recover.
Outlanding into a cropped paddock causing groundloop – forward stick, keep tail off ground to minimise rotation stresses.
Canopy open on launch? Aviate, concentrate on flying, not canopy closure, land ahead if safe, manage energy and extra drag, then navigate and communicate.
Smell insulation burning inflight? Radio call PAN PAN if able, master off, open vents, return and land. If worsening smoke then consider canopy jettison. If even worse, consider bale out.
Bale out scenarios - have you rehearsed how you might exit the cockpit? Have you rehearsed parachute activation procedure?
Club Level Contingency Plans and Responses
Each club and major competition event is required to have Emergency Response Plans. Emergency contact lists are important and necessary, but what about other preventive contingency plans? We might argue that flood or bushfire contingency plans are more likely to be necessary. Severe weather events might require recall or diversion/alternate procedures.
Hangar fires? Clubhouse fires? Ground vehicle fires? What about other scenarios?
Are the non-manoeuvring areas around your aerodrome expanding due to urban incursion or developments, trees or new hazards? Or are new operators mixing it in your circuit areas? How does that affect safe launch and circuit patterns?
New towplanes or winches may require changes in SOPs
New longer wingspan gliders inevitably bring training and conversion implications, but what else could go wrong? You may require new taxiway markers and obstacle clearance measures, with better towing equipment.
So your club has changed a bunch of batteries. Are new charging stations called for? Are chargers being used on the wrong batteries? What about fire prevention and safety, or dropped batteries?
Scenarios and Visualisation
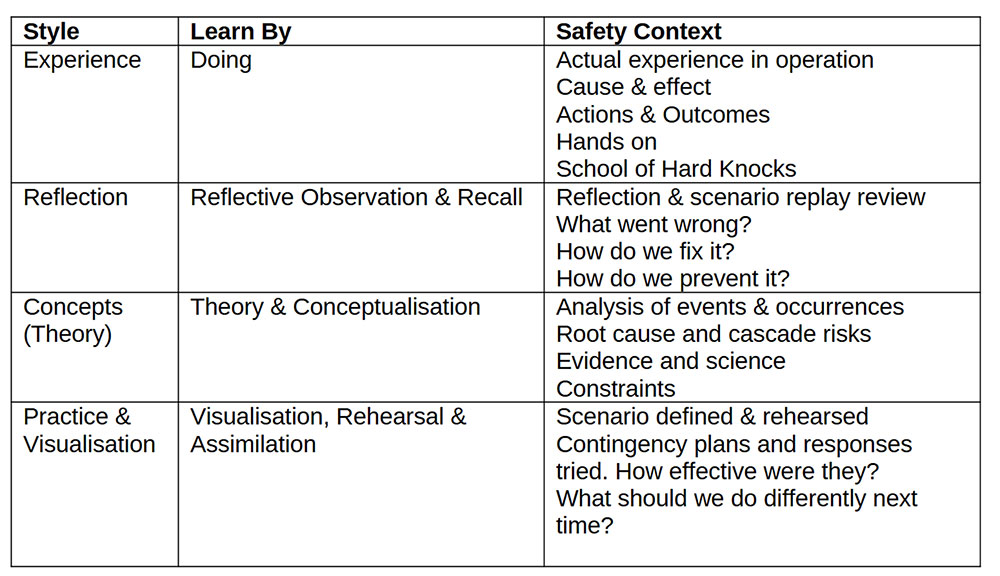
The Training Principles and Techniques (TPT) Manual – accessible in Documents-Training-Instructor training – highlights the Kolb model of adult experiential learning, which also applies in a safety context: Note that these learning approaches can apply to individual pilots and maintainers, members, clubs and all groups and organisations. Visualising the credible new risks we face, or what could happen to us by noting unfortunate occurrences elsewhere, can and should inform our contingency plans and response options.
Hubris is a risk driver. “It will never happen to me” or “we would never do that” are hazardous attitudes. The same applies at organisational levels! “We have great procedures…”
Full Circle…
And so we come full circle.
We are all fallible. We can all make mistakes. I once flew a towplane on a day when I shouldn’t have. It was bonkers. Violent turbulence. Yes, I got away with it but was so close to coming unstuck. Personal judgement errors were primary causes. Then delays, worsening conditions and then I missed a bunch of warning signs. We looked past the pressures and expectations of other people, organisational issues and precedents. We bypassed obvious and foreseeable risks. We boiled the frog! We could have damaged people and aircraft…
Still airborne, I had to do some contingency planning for if or when the approach went wrong – and it did, requiring two go-arounds and modified circuits in rapidly worsening conditions. On the third one I got down okay, but was prepared to go around again. Oh boy, that was scary as!
I replay that flight over, when the instant I was airborne, I knew it was wrong. I visualise what could have gone wrong, nearly did, and what I should do differently in future.
Both feet on the Ground
So I now think about what organisational and personal pressures and circumstances could lead to recurrence, with other people involved. What drives press-on-itis, goal fixation, sunk cost fallacies? What barriers exist leading to a tug pilot saying no? What better decision processes and thresholds should apply? How does a careful sensible safety-conscious pilot end up pushing too far?
The club now has clearer contingency plans about high winds operations and severe weather warnings. We are promoting better use of met forecasts and data, thresholds for limiting operations, tug pilot limits, alternative landing options. We have looked at our risk appetite and thought about credible contingencies. Anyhow, I don’t fly powered aircraft any more…
So, when things go wrong, analysing human, social and organisational factors, operating environments, airworthiness and operations training and systems – all of these require honest evidence-based thinking and careful framing of layers of risk reduction responses, thinking that goes well beyond pilot error. We consider layers that reduce the probability of risks occurring, plus those to limit the consequences. Scenario analysis, contingency planning, options visualisation and rehearsal at both individual and organisational levels can help. It’s worth discussing with your pilot friends and club members.





























